What happens when there are two competing definitions of death, confounding our understanding of the end of life? On 9 December 2013, Jahi McMath, a 13-year-old African-American girl living in Oakland, California, entered the hospital for a tonsillectomy, still one of the most common surgical procedures performed on children and often recommended for sleep apnoea, a condition she had been living with.
Hours after the surgery, Jahi began bleeding, and her mother was worried about the amount of blood Jahi was spitting up. As they begged nurses to call a doctor for more aggressive intervention, neither parent felt that anyone was listening. And then, Jahi’s maternal grandmother, a nurse, noticed that the girl’s oxygen saturation had dangerously dropped. Finally, as The New Yorker reported in 2018, doctors connected Jahi to a mechanical ventilator, or breathing machine. Although the machine was breathing for her, oxygenating her tissues, Jahi continued to decline. Three days after her tonsillectomy, hospital physicians declared her brain dead: that is, with irreversible and permanent cessation of the function of the entire brain, including the brainstem. Observing that Jahi was warm and breathing, her mother didn’t accept their assessment, and the family refused to allow the hospital to withdraw the ventilator. For Jahi’s family, perceptions of racial injustice were at the heart of the tragedy. But what they could not see through their anger and shock was that this was just the most recent development in a half-century of effort to clarify the definition of death.
In the years that followed, Jahi McMath has become a cause célèbre, joining such tragic icons as Karen Ann Quinlan and Terri Marie Schiavo in a movement to take control of the definition and pronouncement of death. These tragic cases, steeped in family pain and political rancour, ask us to consider the true moment of death. Does it arrive, as humans have long held, when the heart stops beating? Or, as modern hospitals and medical science sometimes insist, does it occur earlier, when the brain flatlines, ceasing to produce brainwaves, even as the heart beats on?
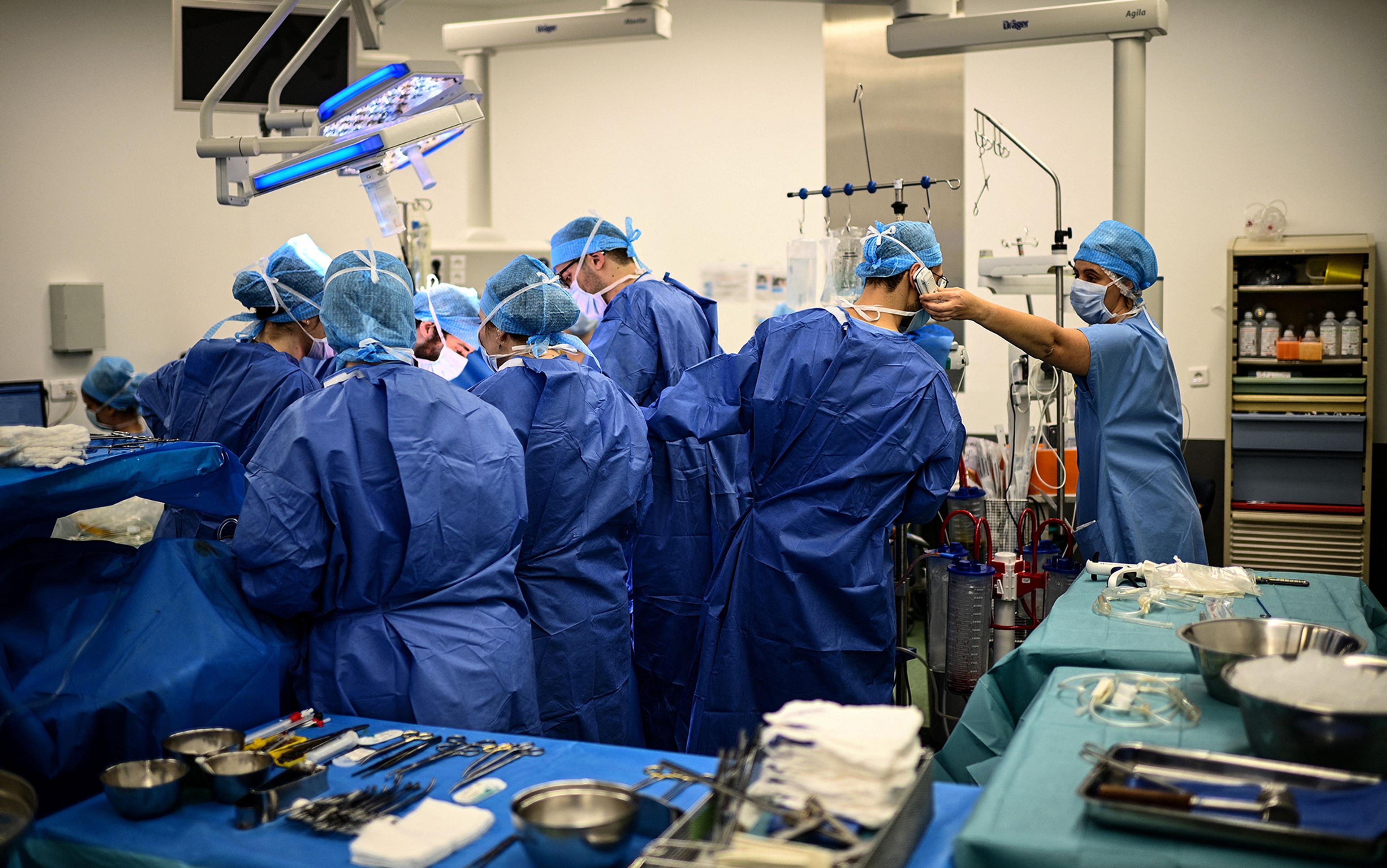
In 1968, a committee at Harvard Medical School invented the concept of brain death, adding a second definition to the classic concept of circulatory death – the permanent cessation of breath and heartbeat, and the irreversible loss of function of the heart and lungs. Patients could now be declared dead while a ventilator kept their lungs ‘breathing’ so their tissues and organs would not also ‘die’. The new notion of death opened the door for a growing number of transplant surgeons to harvest organs still bathed in the nurturing warmth of oxygen and blood. With the chance to save the lives of so many sick patients in need of hearts, kidneys and lungs, the concept of brain death was embraced – but not quite.
The ingredients for a perfect storm had coalesced. The long-ago decision of the committee thrust the rest of us into a battle over the contested territory of death, a battle that still rages. The reason is clear: science cannot tell us how to live. Brain death, which bucks millennia of belief, is not an obvious concept; and medicine’s knowledge cannot encompass the meaning that a family imparts to the consciousness, heartbeat, personhood and life of a loved one. These understandings comprised the ethical stakes in the case of Jahi McMath, and reveal a story about how, despite the efforts of ‘science’, two definitions of death live side by side to this day.
The 20th-century impetus to change the bar for death has a troubling and evocative relationship with the expansive use of the mechanical ventilator. This machine was developed over a 75-year period, first as an improvement over the cumbersome iron lung used to keep polio patients breathing after they lost muscle control. As they were perfected, modern ventilators helped a new generation of surgeons keep patients alive while they operated. By the early 1960s, the ventilator sparked a new opportunity: doctors started using it to sustain life for short or long periods, while patients’ precarious conditions from a variety of diseases stabilised.
Around the same time, transplantation and brain specialists were publishing articles in medical journals suggesting that death should be based on loss of brain function – so that cadaver organs could be harvested for the growing transplantation industry. The ventilator triggered and enabled a pressing medical need: how to keep organs viable and then successfully transfer them from one body into another. Physicians and researchers knew that, in order to make organ transfer legal, ethical and routine, there would have to be a general acceptance of the notion that patients without any detectible brain function could be considered dead.
The Ad Hoc Committee of the Harvard Medical School to Examine the Definition of Brain Death was formed in 1968. Deliberating in private, the 13 men – 10 doctors, one lawyer, one historian and one theologian – put all the stakes on the brain, deciding that those who have a heartbeat and breath (even if machine-controlled) could still be considered dead. Six months later, without public discussion or fanfare, they had produced ‘brain death’, a new category of knowledge and being that would upend everything anyone knew about the end of human life. The committee determined that a person crosses the threshold from life to death when there is irreversible and permanent cessation of the function of the ‘entire brain’, a state that was presumed to preclude consciousness, breathing, cardiac and motor activity. Brain death assumed that there was a clear line to cross. Yet that overlooked a troubling problem: with a ventilator, one could be declared dead while still appearing to be alive.
It was a radical stance that gave rise to an unintended, unprecedented question that continues to haunt us: was the body, pronounced brain dead and connected to a breathing machine, actually alive or dead? No longer would dead mean dead. Death was in this sense doubled. For patients on a ventilator, death could be left open to deliberation, demanding decision-making that then prompts another question: who should have the authority to name death – doctors, hospitals or families?
The brain death of one patient served renewed life in another
To this day, clinical criteria used to make a diagnosis of death often remain at odds with the wider, culturally agreed upon definition of death held by patients’ families. Brain death made death infinitely complicated because a body could be warm, have the colouring of life, and yet be deemed dead by doctors. Death always had multiple medical causes. Now it had multiple medical meanings. Disquiet brewed almost immediately among those philosophers, physicians and others who had been, since the early 1960s, reframing death as a process that occurs over time (because the cessation of different organ and physiological systems happens at different moments) rather than as a discrete event. The Australian philosopher Peter Singer called brain death ‘a concept so desirable in its consequences that it is unthinkable to give up, and so shaky on its foundations that it can scarcely be supported.’ It was, he noted in Rethinking Life and Death (1994), ‘an ethical choice masquerading as a medical fact’.
With death being a multiple and contested idea, organ transplantation proceeded. The brain death of one patient served renewed life in another. And by the mid-1970s, the ventilator had become standard equipment in most hospital intensive-care units, its dark side apparent. It could keep comatose and vegetative persons alive for years, even decades, enabling new forms of life in a grey zone suspended between life and death. In situations where medical tests could not detect brain function, the ventilator was now a source of confusion for a greater number of families and health professionals. Despite the hopes of the Harvard committee, the ethical conundrum spawned by their deliberations continues to reverberate in the bodies of patients, in the agony of families as they try to make sense of what they see, and in the quandaries of medical staff, hospital administrations and sometimes the public.
The saga of Jahi McMath is our most recent example of the ambiguous zone created when ventilator and brain death were paired. The Harvard committee could not or did not anticipate that brain death would become embroiled in our most intimate struggles and national political debates. Or that families would be skeptical of the notion, demand respect and justice on their own terms and a voice in decision-making. Or that hospitals would sometimes struggle with family responses to the idea of brain death. Or that science would complicate matters by defining new conditions of consciousness and coma, indeed, new ways of being human and being alive. Or that the law would become a major arbiter of medical outcomes. Our reckoning with both the tool and the idea of brain death is far from over.
With Jahi McMath’s case, the question of who names and who authorises death became news, just as it had been in earlier examples of patients whose condition had been confusing: in the grey zone, not fully alive but not dead either. However, unlike the prominent examples of Quinlan and Schiavo, Jahi had been declared brain dead. Using the federal Uniform Determination of Death Act (1981), which states that a person who has sustained ‘irreversible cessation of all functions of the entire brain, including the brain stem, is dead’, in Jahi’s case hospital procedure was guided by California law. This law allows families a brief period, no more specific than that, to come to terms with the death, before medical staff disconnect the ventilator.
Incensed, Jahi’s family hired a lawyer and sought a court injunction to delay the removal of the ventilator pending another neurological opinion, which, when ordered, confirmed Jahi’s death. In a show of sympathy for the family, the superior court judge twice extended the deadline for the hospital to remove the ventilator, allowing the family until 7 January 2014 to accept her death or decide how to proceed.
During the days and weeks between Jahi’s hospital-declared brain death and the judge’s ruling, the family made savvy use of social media, crowdfunding and community support. Her evolving story became a media frenzy, with her family joining daily protests outside the hospital itself.
Events surrounding Jahi would continue to unfold in the public sphere and in the courts in the years to come. The media reported that medical staff who had cared for Jahi experienced great distress when, after she had been declared brain dead, the family requested a tracheotomy – a safer, permanent way for her to receive oxygen, and one that would have been used had she been considered alive. Doctors and nurses refused, distraught about acceding to the family by performing a procedure on a dead person. They were also distraught about the way the case was unfolding on the streets.
Jahi’s story remains an open wound in the life of brain death
Then, in early January 2014, with the help of the Terri Schiavo Life and Hope Network, Jahi’s family moved her to a New Jersey hospital where she’d been accepted as a patient. (Only New Jersey and New York had religious freedom laws at the time to allow families to refuse a brain death determination.) They raised more than $58,000 on GoFundMe.com to cover her portable tracheotomy and transportation costs. And, though she was legally dead, Jahi was fed with a feeding tube, given medication, and cared for as a comatose patient for the first time in weeks.
Jahi’s mother thought that, with a feeding tube and tracheotomy, Jahi would wake up and return to life. Her belief appeared partially validated later that year, after moving Jahi from the hospital to an apartment in New Brunswick, New Jersey. There, Alan Shewmon, a neurologist and researcher with years of experience studying minimal states of consciousness, examined Jahi and reviewed her records. He found that, with nutrients and medication, she had improved and was no longer dead.
If only… if only someone on the California hospital staff had been more compassionate, many wondered in the media, and more than several health professionals suggested to me, if only they had explained Jahi’s death in a more sympathetic way and allowed the family more time to accept the tragic event, then perhaps her removal from the ventilator would have been less fraught and her California death certificate would have been the end of her story. If the family had understood a more ‘compassionately’ delivered medical rationale for brain death, would this simpler version of death have prevailed? Possibly, although the problem of the doubling of death remained. Time is of the essence in hospitals, and staff become impatient if families don’t respond to the organisational imperatives of timeliness and efficiency, which in Jahi’s case meant following protocols for a corpse and getting her dead body out of the hospital to make way for new patients.
Here is where perceived (or actual) racial insensitivity coalesced with murky meanings of death. In the family’s opinion, if the medical staff in California had explained what the brain damage had wrought, and if they had taken more time to describe the limits of a tracheotomy when refusing to perform the procedure, then the events that followed could have been different. Jahi’s story, unfolding in a time of neurological advances and acute awareness of racism and rights, remains an open wound in the life of brain death. As Jahi’s mother, Nailah Winkfield, told The New Yorker in 2018: ‘I can’t prove it, but I really feel in my heart: if Jahi was a little white girl, I feel we would have gotten a little more help and attention.’ Sandra Chatman, Jahi’s maternal grandmother, a nurse, seemed to concur. Referring to a doctor she felt had ignored them, she told The New Yorker’s Rachel Aviv: ‘It was like he thought we were dirt.’
The uproar over Jahi McMath is complex and fraught with the decades of turmoil that came before. The ventilator’s dark side caught the public’s attention when Karen Ann Quinlan, aged 21, fell into a coma after mixing Valium with a bout of drinking. She was taken to a local hospital in New Jersey and connected to a ventilator on 15 April 1975. For nearly a year, the media focused on her condition on that machine, unresponsive but not dead. A landmark court case ensued, and the topics of death and medical decision-making moved out of the sequestered hospital world, ushering in our current era of public confusion about what death is, when it occurs, and who says so.
Quinlan was not brain dead. Nor was she fully alive. She emerged from a coma (complete unconsciousness) into a persistent vegetative state (PVS), awake but unresponsive and unaware of her surroundings. To the horror of many, her betwixt-and-between condition was created by the newly routine use of the ventilator, together with attentive medical and nursing care. The young woman drew international attention when her religious parents, after months of soul-searching and discussion with their priest, sought to have her removed from the ventilator, assuming that she would die shortly thereafter. When her doctor and the hospital administration refused, fearing criminal prosecution or other sanctions, her parents petitioned first the Superior Court of New Jersey and then that state’s Supreme Court, which in March 1976 ruled in their favour.
But after the ventilator was removed, Quinlan did not die. To everyone’s surprise, she could breathe on her own. Her feeding tube stayed in place and she remained in an unresponsive condition for nine years before dying of pneumonia in 1985.
The British anthropologist Marilyn Strathern argues that what matters is not whether new ideas and technologies are good or bad in and of themselves but rather how they present and reflect on human affairs. Beginning with Quinlan, the ventilator became a vehicle for new forms of persons and societal responses to those persons. Her liminal status raised an existential dilemma: what to do, for something had to be done, about this kind of person. Discussions about who is in charge of such a person and what constitutes a life worth living forced many to ask: what, in the face of betwixt-and-between patients, are the goals of medical treatment?
Following closely on the heels of Roe v Wade, the landmark US case that ultimately protected a woman’s right to choose abortion in 1973, Quinlan’s case opened heated deliberation about what kind of life has value, and who gets to decide. The case gave the courts a large role in shaping right-to-die law. The New Jersey Superior Court judge ruled that the question of Quinlan’s removal from the ventilator was a medical one, stressing that the professional norm and standard of care was to provide life-extending treatment. At the time, the court felt an obligation to protect medical decision-making, and they affirmed the medical paternalism of the era. The family was to have no say in the matter.
In rejecting the lower court’s decision, the New Jersey Supreme Court placed decision-making authority squarely in the hands of the Quinlan family, breaking ground in several ways. It acknowledged that an unresponsive patient’s right to privacy could be claimed on her behalf by family members through ‘substituted judgment’, even when the patient’s wishes could not be discerned. In doing so, it opened decision-making to families. It also acknowledged that the withdrawal of treatment hinged not on mere biological survival, but on the probability of the person’s return to some form of aware, conscious state.
Brain death enabled organ transplantation and spurred the growth of a new medical-industrial complex
The case had an enormous ripple effect. It contributed to patient and family activism about end-of-life interventions. It opened the way for the hospice movement to gain support in the US. It gave rise to the use of the living will and advance directives. It brought into medicine a new language of rights and public policy. It raised new questions about the goals of the ventilator and of medicine, about what kind or degree of life equals being alive, and what the role of the law, the family and the medical profession should be in fostering or ending that life for any one person. Finally, the creation of betwixt-and-between persons on ventilators fostered the need for specialised hospital units, care providers in those units, and new administrative arrangements and insurance mechanisms to pay for the units and the specialised care.
Many participants in today’s debates about not-quite-dead-but-not-fully-alive persons seem unaware of its history. I’m surprised at how many medical students and young doctors I speak with have not heard of the Quinlan case. Yet the ventilator that enabled her situation and the overarching question of who gets to decide the time for death are by now ordinary elements of clinical work, as well as family and societal angst. But being ordinary does not mean ‘problem solved’, and the ventilator continues to provoke troubling and sometimes public cases that highlight our ongoing inability to come to terms with the definition and control of death.
Twinned with the ventilator, brain death elicited new forms of thought, new kinds of persons, and it changed institutional arrangements too. In 1981, with brain death enshrined in the US law as the federal Uniform Determination of Death Act (similar European legislation followed), the uneasy coexistence of two kinds of death proceeded to reorganise medical practice. Hospital protocols regarding how to diagnose, discuss and respond to brain death were created in tandem with developments in the mushrooming organ-transplantation enterprise. Formal diagnostic tests had to be created, standardised and shared among institutions and medical governing bodies. The doors opened for organ procurement to become a multimillion-dollar industry with its own rules and regulations about how and when to approach dead persons’ families, and who should discuss donation with them (not the physicians who would transplant organs). Jobs were created for healthcare professionals who would ‘procure’ the organs and move them from place to place. Insurance had to cover the procedures and the moves. Airlines became involved.
In 1984, the US Congress passed the National Organ Transplant Act, calling for a ‘national network to coordinate the allocation of organs and collect clinical data about organ donors, transplant candidates and transplant recipients’. Other nations followed, and the transplantation enterprise contributed to the growth of bioethics as a profession, because a system that allowed for the removal and placement of human organs required judgments about fair distribution and allocation. Fairness, however conceived, requires periodic review in light of shifting societal values and norms, changing race and age demographics, and the growing rural-urban gap in prospective recipients’ waiting times for organs.
In all these ways, brain death was routinised and normalised. The protocols, personnel, labour and financial arrangements solidified brain death as an actual thing, a reality on the ground shaping hospital work and budgets, national networks, medical specialties, and patient and family decision-making about organ donation. Brain death enabled organ transplantation and then spurred the growth of a new medical-industrial complex.
Despite the normalisation of brain death, the debates never stopped. How can we deal with the ambiguity of bodies that are arguably neither persons nor cadavers? And are we asking organ donors to die twice?
After Karen Ann Quinlan, neuroscientists redoubled their study of states of consciousness, provoking still more murkiness about the clear line between life and death. During the 1990s, a more powerful neuroimaging tool, functional magnetic resonance imaging (fMRI), was able to reveal changes in brain blood flow almost as they occurred. The fMRI, along with years of careful observations of seemingly unresponsive ventilator-supported patients’ cerebral reactions to stimuli, established categories of brain activity and consciousness never previously observed or named.
Shewmon, a leader in this new field of study, used data accumulated from patients declared brain dead who were sustained on ventilators to study what he called ‘chronic brain death’ in those persons who showed prolonged survival after a brain death diagnosis. In a 1998 study, he showed that, while some patients’ conditions mimicked brain death, they retained sufficient bloodflow to prevent brain deterioration, increasingly prevalent with advancements in ventilator technology. What most people thought was a definitive event could, in this view, be a prolonged condition – death could be chronic.
These findings raised at least three thorny issues. First, with more diagnostic categories found through observation and imaging techniques, certain patients who had been considered brain dead were now thought to be severely impaired but not dead. Second, the observation that in certain cases brain death is not irreversible led to doubt about the diagnosis. Finally, a problem present since 1968 became glaringly obvious, and the saga of Jahi McMath drew broad attention to it. Writing in 2005, Winston Chiong, a neurologist and bioethicist at the University of California, San Francisco, said: ‘Even after the standard battery of diagnostic tests for brain death has been fulfilled (including documentation of coma, the absence of brainstem reflexes, and the absence of respiratory effort), many brain functions persist – including such presumably integrative functions as hormonal secretion and thermoregulation.’
Who decides what kind of consciousness is worth sustaining and who should count as dead?
In 2002, enabled by increasingly powerful imaging tools, neurologists added the ‘minimally conscious state’ (MCS) to the lexicon – in order to account for patients who did not fit any existing labels and to further refine the older designation of persistent vegetative state. Patients in MCS show intermittent awareness of themselves and responsiveness to their environment. Subcategories have since been formed, including ‘minimally conscious plus’ (MCS+), ‘minimally conscious minus’ (MCI-), and E-MCS for ‘emergence from the minimally conscious state’. Such diagnoses categorise patients’ brain functions more specifically than ‘persistent vegetative state’, but further complicate the relationship between consciousness and life because they introduce new ways of being human.
One neurologist I spoke with in 2018 asked: ‘To what end do we make these discrete diagnostic labels?’ He noted that the added categories don’t lead to better predictions, only less prognostic certainty. ‘That’s what we want to be better at, but we’re not there yet,’ he added, inferring that, for some families, the burning question is whether the diagnosed state of consciousness of their loved one is ‘good enough’ to keep the person alive.
We are left asking: can a diagnosis of brain death be accurately obtained? Can its criteria be definitively mapped? There are those who claim that accuracy is possible when hospital protocols are strictly followed and technologies are used properly, reasoning that it is a matter of biology, and that, if science can identify kinds and stages of consciousness, then clear diagnosis, prognosis and decision-making will follow. Far more problematic is the fact that, so far, the ability to finely hone brain-function states has not clarified the social and policy problem of who decides what kind of consciousness is worth sustaining and who should count as dead – that is, whose ventilator support and feeding tube should be withdrawn.
Controversy on this matter has only increased, and the newer categories of being, including minimal consciousness, have further complicated civil rights. Right-to-life and right-to-die debates have grown more widespread, contentious and violent. Some think that any form or degree of brain activity should be medically supported. Others counter that ventilator support can be withdrawn ethically from someone who is ‘as good as dead’ because ‘higher brain function’ (the capacity for self-awareness and thought) is absent. But what constitutes ‘higher’ capacities can be viewed differently by medical personnel and by a patient’s family. And, since Quinlan, high-profile cases of persons betwixt and between life and death reveal public anxieties about determining what a high-enough brain function should be in determining death or the preservation of life, and what counts as meaningful-enough recovery to demand or ensure life-sustaining treatment in cases of severely disordered consciousness and function. Jahi McMath’s is only the most recent example.
The dilemma of who should decide whether a brain-injured life is worth living reached the US Supreme Court in 1990 with the case of Nancy Beth Cruzan. In 1983, when she was 25, Cruzan was diagnosed in a persistent vegetative state following a car accident. She breathed on her own but required a feeding tube for nutrition and hydration. After several years witnessing no improvement in her condition, her parents asked the hospital to remove the feeding tube, allowing their daughter to die. The hospital refused, and the case wound its way through the courts. In the end, the right for patients or their surrogates to refuse any and all medical treatment became federal law, though the US Supreme Court limited that right by rejecting the right to privacy that had determined the Quinlan case. The court determined, instead, that individual cases could be subject to state regulation. A Missouri court ruled that Cruzan would have made the choice to disconnect the feeding tube, and she died two weeks later.
Could the authority to control the time of death, or contend meaningful-enough recovery and life, be resolved in a battle of persuasion between family members, carried out in the courts? Indeed, it was. In 1990, aged 26, Terri Marie Schiavo had a cardiac arrest. The cause was never definitively explained. She was diagnosed as being in a persistent vegetative state and never regained consciousness. In 1998, her husband sought a court order to allow her feeding tube to be withdrawn, which, he hoped, would allow her to die. The Florida court determined that the tube should be withdrawn, based on their assessment of Terri’s stated wishes. Her parents baulked at the idea, initiating a prolonged legal battle with her husband that wound through the Florida state legislature and courts (which repeatedly upheld the initial ruling) to the US Congress. The family battle brought media and political attention to opinions about her condition. In 2005, a US circuit court judge finally ordered the tube removed, and she died two weeks later.
Advances in neuroscience up to the time of Terri’s death heightened the rancour between her husband and her parents. Their fight – especially regarding possible reversibility and the new categories of consciousness – fostered the most protracted public controversy yet about diagnosis, prognosis and whose rights have authority. Cable radio talk-show hosts, elected officials and ordinary citizens took sides, and aired them vociferously in the media: Terri was alive, brain dead, as good as dead, permanently vegetative, minimally conscious. She would recover, would never recover. The husband, no, the parents, should win in court. All the talk further entrenched and strengthened the right-to-life and right-to-die movements. One neurologist-ethicist remarked: ‘It used to be enough for a neurologist or neurosurgeon to write a note in the chart grimly recording the patient’s neurological exam, and then concluding with the global statement: “No hope for meaningful recovery.” It can no longer be so simple.’
Though doctors who examined Terri repeatedly affirmed her persistent vegetative state, the politics of mutable diagnoses made it impossible for the case to settle. The deliberations in the Florida state legislature in the early 2000s and in the US Congress in 2005 became part of the expanding conversation about brain death. Two elements fuelled the controversy: the uncertainty created by the new diagnostic categories, and the heightened tensions between right-to-life and right-to-die groups. Who defines ‘meaningful recovery’ was a core question in the Schiavo case. The dilemma of how to define a life worth living was ignored beneath the uproar, which rose again with the case of Jahi McMath.
In August 2014, from their apartment in New Jersey, Jahi’s family talked and read to her while caregivers worked round the clock. Jahi’s mother remained convinced that her daughter was responsive to gentle commands such as ‘lift your right hand’ and, ultimately, Shewmon agreed. Jahi had also begun to menstruate. Legally dead, medically not dead: Jahi’s condition was vexed.
Do we want judgments about death decided by judges or juries?
In 2018, Jahi’s family was preparing to take her home to California where they were pursuing a lawsuit against UCSF Benioff Children’s Hospital Oakland, where the original surgery took place. A California judge had decided that a jury would determine Jahi’s status as either dead or alive. But on 22 June 2018, before the trial began, Jahi died following liver failure that led to a cardiac arrest. We will never know how the court would have decided. The family declared her dead, and acquired her second death certificate. She was buried in Oakland in a well-attended, well-publicised funeral.
It seems impossible, now, to settle on what death is. I’ve watched brain death evolve, and consider it one of medicine’s most thorny notions. Its definition and criteria continue to be debated, even as new imaging technologies emerge. In Jahi’s case, a combination of factors – a heightened attention to racism and rights in healthcare delivery, new diagnostic tools, a refined neuroscientific classification of states of consciousness and increased family activism – begin to challenge not only the concept but the entire social and technological construction of death itself. That cluster of developments has opened discussion, currently underway in medicine and bioethics, about greater family participation in naming death and authorising its time.
Leading the way are two bioethicists, Robert Veatch of the Kennedy Institute of Ethics and Lainie Friedman Ross, also a physician, of the University of Chicago. Together, they argue for choice and a place for conscientious objection against ‘a uniform definition of death that would permit patients (or their next of kin) to have discretion within certain limits to choose which definition of death should be applied to them based on religious or philosophical beliefs’.
Over the course of 50 years, no one has managed to stop the audacious invention of brain death from taking medicine by storm. For way too long, the chutzpah of the concept has been buried beneath the protocols and rules that ensured its reality and the guidelines and practices that addressed, as best they could, the dilemmas that death provoked.
Since it was first conceived, brain death has acquired a life of its own, joining the stem cell, the embryo, the persistent vegetative state and the cadaveric organ donor as a biomedically generated form of life at the edge of what we collectively understand life to be. The debates over each controversial case fade with time, but the life of brain death remains a magnet for activism and debate. Choice in the matter of death has its echo in our national struggles over abortion. Issues of resource allocation and healthcare disparity loom large as well. And the central questions remain: do we want judgments about death decided by judges or juries? By social protest? Or by ourselves, our families, and those we love? Why wouldn’t we want families to decide if their loved one is as good as dead or is, alternatively, alive enough to be worthy of the medical tools available to sustain that life?
Brain death emphasises our stake in this dilemma, and everyone is a stakeholder. Any one of us might be confronted with two (or perhaps more) definitions of death and be confused by their competing claims. Yet perhaps despite or because of all of this, the idea of brain death shows us something about what we yearn for, what we can and cannot accept, and what love and politics look like in extremis and under the microscope of this concept’s dystopian logic.